Report on: The "Sastipen Network Information System
CHAPTER I: INTRODUCTION, OBJECTIVES AND PROCEDURE
1. INTRODUCTION:
In this document we present the work done on the creation of an "Information System on the Evolution of the Situation within the European Roma Population with regard to Drug Dependencies and other Related Problems" as specified in the last section of objective 5 of the European Project Santé et Communauté Tsigane of the Sastipen Network (European Network for Drug Abuse and HIV/AIDS Prevention in the Rom Community). The partners comprising this network are: Asociación Secretariado General Gitano (Spain), Unión Nationale des Institutions Sociales D´Action pour les Tsiganes-Etudes Tsiganes (France), Red Europea Anti-Pobreza (Portugal), Coordinamiento Nazionale Comunnità di Accoglienza (Italy), Information and Support Center for Gypsies (Greece), T3E (UK) Race and Drugs Project.
The European Project that the ASGG as coordinator and the above-mentioned partners have been working on since 1995 is striving to continue to meet the health needs of the Roma communities, to promote awareness actions focusing on the Roma community itself, on drug services and on the different responsible government administrations. It is also attempting to implement specific measures aimed at caring for a group of people hurt by the phenomenon of drugs and that until now has received very little attention. Within this broad framework, one of the specific actions proposed is the creation of an information system on the health status of Roma throughout a number of different European countries.
The need for a tool of this nature stems from the difficulty in finding ongoing and systematic data on the health status of the Roma and the incidence of problems related to the phenomenon of drug dependency. The existing data is piecemeal, dispersed and difficult to find and is of no use in the implementation of interventions and the creation of policies and programs that are tailored to the different realities of the Roma communities.
This system is designed to obtain ongoing and updated information on drug dependencies and the health status of the Roma population in the network partner countries. Moreover, it would be useful to have a tool that is capable of evaluating the impact of drug and health policies on this segment of the population. In short, the aim is to acquire updated information that can be used for diagnostic purposes and in the design of interventions tailored to meet the health problem needs facing these communities. In order to accomplish this and as is explained in the section "actions envisioned" within the above-mentioned project "Health and the Gypsy Community", the Secretariado General Gitano has hired the Criteria Grupo de Evaluación (Criteria Evaluation Group), an external entity specialised in these subjects (please find c.v. attached as an annex document) that, as an expert on methodology and in collaboration with the working groups in each one of the member countries, is in charge of the design and the implementation of this system.
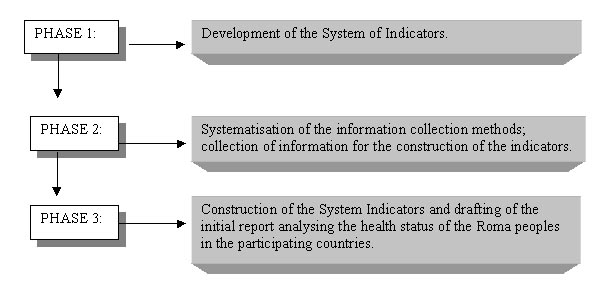
Originally and in line with the initial design set out in the project Health and the Gypsy Community, the following three phases were defined to be followed in the elaboration of an information system: an initial theoretical/methodological phase, focusing on the definition of objectives, instruments and indicators; a second phase dealing with the implementation of the system in each one of the partner countries through the working groups; and finally the drafting and publication of an annual report containing the information obtained.
2. OBJECTIVES
This system is designed with the objective of acquiring updated and systematic information on the health status of the Roma in Europe; information that allows for the design of action plans and programs tailored to the needs of these groups. Furthermore, the idea is to use this tool to evaluate the changes that occur within this sector of the population.
In order to achieve these aims and to implement an efficiently operating system, much work still needs to be done and we have only just begun with the definition of more precise goals. In this chapter we are going to describe the objectives of this initial phase of implementation; a phase that is mainly characterised by the search for consensus regarding the theoretical and methodological characteristics that define the information system.
The objectives established for this first year are:
3 . PROCESS/ PROCEDURE
The following three phases are distinguishable in the procedure followed in this first period of system development:
CHAPTER II : THE INFORMATION SYSTEM
1. RATIONALE BEHIND THE INFORMATION SYSTEM SELECTED
This project is in response to a request made by the ASGG for an Information System guaranteeing the supply of unified data at the European level allowing for longitudinal (long-term) and transversal (comparative) analyses of the health status and health-care situation of the Roma population in the participating countries. We were called upon to create a system for the observation, diagnosis and drafting of recommendations for action in this field in accordance with the project "Health and the Gypsy Community" (doc. Health and Community, objective five).
In a strict sense of the term, an information system is defined as a set of procedures the purpose of which is to systematically collect data on a pre-determined series of variables. Information systems are characterised by the organisation of notifications around a central unit responsible for the collection, processing, analysis and subsequent elaboration of the data.
Information systems are designed in relation to a set of indicators that has proven helpful in shedding light on the object of the study. An indicator is defined as a quantitative variable or set of variables that allows for the identification of changes taking place with respect to a particular phenomenon.
It is therefore of fundamental importance to correctly select the indicators that will form part of the system; indicators that have demonstrated their validity and reliability with regard to the phenomenon to be measured.
A good example of a system of indicators related to drug-dependencies in the case of Spain is the Sistema Estatal de Información sobre las Toxicomanías – SEIT (State Information System on Drug Abuse). This system is based on three epidemiological indicators: commencement of treatment, emergency room visits and mortality. These indicators are traditionally used in epidemiological studies and have proven to be useful in the identification of the incidence and prevalence of the evolution of drug abuse.
In the case at hand, it is our view that we are creating a broad-based information system and not one strictly based on the development of epidemiological indicators.
The indicators are the reference but the information can be broader. This means that in addition to the information that can be obtained from the established indicators, other more qualitative information can be procured which will shed further light on the health status of the Roma, their habits and the proper interpretation of the indicator with a view to facilitating its definition and, if need be, its future development. This combination of methods and flexibility in the system is mainly due to the fact that the obtainment of epidemiological indicators in the case of the Roma population presents a great many difficulties which are not so much related to the selection of suitable indicators (there are a number of indicators that have proven effective in the field of drug dependency and for health-related aspects) but rather to how to go about collecting this information especially if this is to be done in a systematic manner.
In the case of Roma, the greatest difficulties are related with the collection of information because in light of their nomadic tendencies as travellers in England or their status as refugees in Italy or the conditions of poverty and marginality which characterise the lives of many groups, systematic and ongoing data collection becomes very difficult.
Furthermore, the Roma people as such do not identify with any of the health systems operating in Europe today meaning that the normal statistics do not shed any specific light on this issue.
Faced with these difficulties, the information system that we propose has some peculiarities compared with more traditional designs. The final objective is the same as for the more traditional designs: to offer reliable, updated and ongoing data on the health status of this sector of the population. The invisible nature of the situation does not make it any less serious and points to the need to make adjustments to programs so as to be better able to deal with specific problems.
It should also be pointed out that the system described in the following chapter is based on the ongoing collection of a set of information on several pre-determined indicators, using a variety of data collection procedures, ideal for use within each one of the partner countries and that provide periodical information on the health status of the different Roma communities; i.e. used to observe, make diagnoses and draft recommendations for subsequent action.
2.2. CHARACTERISTICS OF THE INFORMATION SYSTEM
With a view to setting up a Health Information System, our study proposal focused on the design and development of a system of indicators in the following four areas:
1.- Drug-dependency and associated diseases.
2.- Health habits, hygiene and nutrition.
3.- Access to and use of mainstream health resources.
4.- General / global health.
Aware of possible difficulties in the gathering of information for the development of indicators, we have come up with four strategies that will be implemented sequentially:
The purpose of implementing this set of strategies is to obtain information on the health status of the Roma people as well as to implement different sources of data collection to feed the system. The indicators proposed can also be used as references around which the data is collected. A variety of methods can be used and the idea is to gradually construct a whole system.
The system’s development phases are as follows:
2.3. HEALTH INDICATORS SELECTED FOR THE ROMA COMMUNITY
The selection of indicators is no easy task and one must never lose sight of the final aim of the system of indicators being built. Based on that final aim, the indicators were selected using the following criteria:
1.- Importance and relevancy of the indicators for health issues within the Roma community.
2.- The existence of the indicator in the non-Roma community.
3.- The ability to gather the information needed for the development of the indicator by means of one of the methods proposed.
4.- Balanced coverage of the marked areas for the establishment of a system of indicators.
The final objective is that of setting up a system of indicators that is broad enough in number to cover the objective but not so extensive so as to require undue effort. We now turn to the indicators.
The indicators selected and "possible" sources of information for gathering purposes as proposed to all of the partners:
Block 1 Drugs
1. Number of individuals treated for drug problems.Block 2 Health habits, hygiene and nourishment
1. Consumption of fats, proteins and calories (percentage of the average Roma diet).
Block 3 Access to mainstream systems
1. Percentage of births in health centres.
Block 4 Global health indicators
1. Percentage of stillbirths.
2.4.- DOCUMENTATION SEARCH RESULTS
ANALYSIS OF THE INDICATORS
BLOCK 1: DRUGS
In this block we propose a few changes. The data that we have collected comes mostly from two types of sources: drug centres and prisons. Neither of the cases is characterised by a systematic collection of data but rather were ad hoc studies carried out at a given time by the professionals working n these services or centres.
There are also some data on the consumption of technically legal drugs covering the general population or a specific neighbourhood but this was not one of the indicators included in the initial proposal.
We now propose some changes with regard to the last proposal. We changed indicator number 4 of those proposed and we now list it as follows: Drug consumption (legal or illegal). We also broadened indicator number 1 with the socio-demographic characteristics of those being treated for drug dependency.
Very little data was found due to the fact that none of the multi-centre information systems register the ethnic group to which the patient belongs. We have, however, been able to find some data stemming from a specific published scientific study or master’s thesis.
We have one study that we feel is significant in its field carried out in the city of Coruña in Spain. Data was collected in the Coruña Drug Dependency Treatment Unit on Roma individuals treated as part of a study on the incidence of HIV/AIDS in that sector of the population. Eleven years worth of data was analysed for that study (1984-1995). In this centre close to 200 request for treatment were made by Roma while the estimated Roma population residing in the city is around 2,000. They had the following characteristics:
As is the case with all of the indicators selected as we will see, we understand that generalisation of the data is a problem. These data can, however, indicate a very serious drug dependency problem, at least in the case of some groups of Roma that may not yet turn to mainstream health services for help. In this case it can be observed that the demand was mostly for methadone treatment that, in principle, is the one less culturally influenced from among traditional treatments.
This same study points to the importance of HIV/AIDS infection within the Roma, drug-dependency population.
We were not successful in finding any information whatsoever regarding this indicator. This clearly requires an ad-hoc study or agreements with health authorities to collect this information on a regular basis in hospitals and forensic services. We have not eliminated it because it is our view that it could be a useful and objective indicator of evolution if it could be collected in a reliable and systematic manner.
With regard to this indicator, most of the available data is on the prison population in Portugal and Spain. The following is the most relevant:
In the Porto Penitentiary Centre (Custoias), the male Roma population accounts for 3.4% of the total number of inmates with the following age distribution:
50% 16-20 years of age
9.7% 21-25
15.9% 26-35
4.9% 36-40
17.1% Over 40
2.4% No information available
75% of the arrests were related to drug trafficking: 70.7% for drug trafficking and 4.9% for suspicion of trafficking.
61% of the Roma inmates suffer drug dependency problems although only 7.5% have participated in the Support Program for Drug-dependent Inmates.
These figures show that today a high percentage of the Roma inmate population is involved in the trafficking and consumption of drugs. This information coincides with clinical data: 69% have had or still have the hepatitis B or C virus and 12% are HIV/AIDS seropositive; high-percentage pathologies in the drug-dependent population.
We also have another study on incarcerated Roma throughout the whole of Portugal. As an ethnic group the Roma account for 5.5% of the total inmate population, relatively higher in comparison with other groups. The majority are repeat offenders and/or members of the same families which leads us to believe that they are not representative of the entire Roma population but rather of a sub-group. Of these 79% are men and 21% women.
In this case, 40% of the male inmates were drug-dependent, a figure that indicates a close relationship between drug consumption and prison sentences. This figure falls to 3.1% in the case of women. The relationship that these Roma men and women have with drug trafficking, however, is much stronger:
This indicates a close relationship between women inmates and drug trafficking (although the relationship with consumption is much weaker) and a relatively higher relationship between drug trafficking by the Roma when compared to non-Roma. These figures may be relative, however, because there may be greater police and court pressure on individuals from this ethnic minority.
In Spanish prisons, 25% of the women inmates are Roma (while it is estimated that they account for 1,4% of the total Spanish population). 49% of the sample of 290 Roma women imprisoned in Spanish jails was or had been a consumer of illicit drugs. This percentage rose to between 60 and 65% in the case of those under 30 years of age. This relationship between Roma women inmates and drug consumption is significant because in many of the reports that we have gained access to, the consumption of drugs by Roma women is not recognised, not even in the case of legal drugs (alcohol and tobacco) as we will see below and as was the case with the Portuguese prisons.
We have data on the consumption of alcohol and tobacco in some groups. We will now take a look at the most significant information.
Here we will analyse data on equipment, vaccination records, etc. taken from an in-depth study done on four sites in Andalusia (somewhat outdated being from 1985 but one of the most complete studies that we came across; figures are an average of the four sites).
MEN
Alcohol 76.2%
Tobacco 83.6%
It is hard to determine the reliability of these figures as is generally the case particularly with alcohol, but they do show a high or almost generalised use of alcohol and tobacco among Roma men. In the case of women, no alcohol consumption was admitted and only two sites recognised a very limited number of cases of tobacco use. We feel that this clearly indicates a more moderate consumption of alcohol and tobacco on the part of women (although it is assumed that this is on the rise), as well as a tendency to conceal this consumption in light of social stigmas.
In the case of illicit drugs, we have very little data except that relating to the inmate population and is therefore not very applicable to the population as a whole.
In the Porto prison analysed, 61% of the inmates had had drug dependency problems although only 7.5% had actually turned to the prison support program for help.
As is also the case with the non-Roma population, it appears that there may be a relationship between the consumption and trafficking of drugs and criminal activity and prison sentences. It is assumed that this relationship is applicable to a sub-group of the population that would be interesting to identify. In the case of the non-Roma population, it appears that drug-dependency (and the consumption of drugs in general) is a phenomenon that transversely affects all social classes, i.e. marginated groups consume to the same degree as integrated segments of the population (independent of the seriousness of the problem in each case). It would be interesting to discover the degree to which these problems have also made their way into all groups of Roma or if one of them appears to be more permeable both with regard to consumption as well as trafficking. As was mentioned above, women tend to be incarcerated more for drug trafficking and this is probably due to the fact that if trafficking is a family economic activity, women play an integral role while the consumption of both legal and illegal drugs is culturally taboo for women.
What does appear to be true is a high incidence of consumption in some family environments. In a study done in Santiago de Compostela on the incidence of drug-dependency problems within families (survey of 84 people), the following was discovered:
Spouse or partner 13.1%
A sibling 36.9%
A brother or sister-in-law 34.5%
An aunt or uncle 41.2%
A cousin 85.7%
These figures would seem to indicate family environments that are quite affected but it should not be forgotten that families are large and normally close-knit; a fact which could affect the data.
Along these same lines, half of the men surveyed stated that they had or had had some sort of drug problem while none of the women admitted the same.
BLOCK 2: HEALTH HABITS, HYGIENE AND NOURISHMENT
Here we propose a number of changes with regard to the indicators. With respect to nourishment (indicator number 1), the studies that we found offer information mainly on children’s height and weight, obesity or symptoms of malnutrition probably due to the fact that this is information that is more objective and easier to obtain. This indicator could therefore be changed and include this other type of information instead of the food products consumed.
Indicators 3 and 4 have been eliminated. The first referred to childhood accidents but we found no data and it seemed to be a secondary indicator that could later be added once the primary indicators are consolidated.
As far as indicator number 4 is concerned (percentage of Roma who have general medical, dental and gynaecological check-ups), we feel that it is covered in Block 4. Although conceptually we included it here under health habits, the lack of data that we were able to find justify its being excluded here.
And finally, the wording of number 5 could be changed. Here we feel that we should include the percentage of standard and sub-standard housing including shanty-town housing, tents, pre-fabricated hovels, provisional housing, over-crowded housing, etc. We feel that this would facilitate the gathering of data although it is also true that we have quite a bit of information available (electrical installations, water, heating, etc.).
1. Consumption of fats, proteins and caloriesAs has already been stated, we believe that a new format must be found for this indicator relating it more with weight, height, obesity and symptoms of malnutrition thus allowing for more quantitative-type data. We will therefore use the heading Nutrition and include data on the consumption of fats, proteins and calories, children’s height and weight, obesity and symptoms of malnutrition.
The data found in this search and which was presented in the most thorough way corresponds to the four sites in Eastern Andalusia referred to above. Here we have weight and height figures on Roma children. It was discovered that between 48 and 60% were within the average percentile ranges corresponding to the general population when it came to weight and between 52 and 60% as far as height is concerned. The greatest differences vis-à-vis the general population were found in one of the sites regarding nursing children under two years of age.
With respect to adults, the most significant finding was a high percentage of obesity cases, particularly among women, and occurring at younger ages than is usually the case for the general population. Figures indicate an obesity rate for women of 50% with high percentages for women under 40 years of age as well. Percentages for men are lower but did reach the 30% level in the case of certain groups.
Depending upon the site, different forms of malnutrition were discovered in up to 15% of the individuals studied.
In other studies more qualitative data was found that seem to indicate that the Roma diet is rich in carbohydrates but poor in proteins and fats. Improper eating habits were discovered both in relation to nutritional balance as well as meal schedules or other behaviours such as the lengthening of nursing to 2 or 3 years subsequently being directly replaced by the normal family diet. Generally speaking, this diet lacked fruits, vegetables and proteins such as fish, milk products or legumes. On the other hand it was particularly dependent on starch, eggs, pork meat, processed sandwich meats and sweets.
2. Percentage of children vaccinatedThis is one of the indicators for which we have the most information gathered from different locations and for different pockets of the population. The data vary according to the different populations but we feel they indicate increasingly broader coverage to the same degree that other data show increasing mainstream health coverage.
In the four sites in Eastern Andalusia that are characterised by a relatively marginal population, the average figures are as follows (remember that these figures are from 1985):
Complete battery of vaccinations 10,2%
Incomplete vaccinations 46,6%
No vaccinations 42,9%
Tuberculosis vaccination 10,4%
It should be pointed out, however, that the data were quite disperse and in one of the sites the percentage of incomplete vaccinations reached the 73% level with complete vaccinations at 18%. In the worst site, only 4.6% had all of their vaccinations and 29% were incomplete.
Other data collected from two neighbourhoods in Seville (also in Andalusia) show the following (1991 data):
- Vaccinations for children under 7 years of age 77.6%
- Between the ages of 7 and 14 63.1%
This seems to confirm a progressive improvement in the situation.
And finally we present the vaccination percentages of the total Portuguese Alentejo population (1992):
YES 65.6%
NO 26.8%
INCOMPLETE 7.7%
It could be concluded that vaccinations are far from being generalised throughout the Roma children’s population although in some places they have reached relatively high percentages of coverage.
3. Number of domestic accidentsVery little data was found on this indicator. Our only source of information was a study on burn risk factors affecting children carried out by an Athens hospital in 1998. Seventeen out of 239 of the subjects studied (7.1%) were Roma or children from groups of recent immigrants but we have no information regarding the reference population of the hospital that did the study. The burns were associated with the children’s activities. Walking barefoot and being in kitchens were the two behaviours that led to the greatest number of burns.
This indicator has been eliminated in the new proposal in light of the difficulty in obtaining reliable data and given its secondary importance.
4. Percentage of Roma who have general medical, dental and gynaecological check-upsDespite its conceptual difference, this indicator is closely related to those of block 3 and has therefore been eliminated. Moreover, the data that we obtained refers to the frequency of hospital or health services visits with relation to the emergence of a specific problem but have little to do with routine check-ups which is what is being searched out here and concerning which we have hardly any information.
What can be affirmed is that the rate of visits to hospitals and health services is much higher than that of the general population and this is most likely due to the greater number of health problems and a conception of health care more in tune with medical intervention than with prevention.
5. Housing utilities
This is probably the indicator on which we found the greatest number of studies and data. Despite this fact, we think that its format should be changed in order to take stock of the different types of housing and not concentrate so much on utilities. This indicator is very much affected by the type of population group to which the data refer and when marginal groups are the object (as is the case with many studies) it goes without saying that household utilities will be lacking but it would be helpful to know the relative importance of these groups with respect to the entire Roma population in a particular geographical area.
In a 1995 study on Roma in Andalusia we found that 53% of the Andalusian Roma lived in government housing projects and recently constructed areas and 85% had been living in the same municipality for more than 15 years. We are therefore dealing here with an established group without general access to standardised housing.
Continuing with Spain, in the Community of Aragon (approximately 8,000 people of Roma ethnic origin) their situation could be considered standard as far as housing utilities are concerned.
Water 89%
Electricity 95%
Heating 71%
The situation is not the same everywhere, however. In the city of Sofades (Greece), where approximately 2,000 Roma reside, a study was done involving 419 homes (270 families, 1,700 individuals). It was found that 18.8% were of standard construction, 19% were of brick or cement block, 29.1% were made of wood and aluminium, 31.5% were made with plastics and 1.4% lived in tents or automobiles and 34.9% were legally connected to the electrical system thus indicating a low level of utilities and overall comfort (1994).
Continuing with Greece, we have a study on 26 shanty-town settlements where 2,500 families resided and the situation differed among the different settlements:
5 out of 26 settlements had been closed down.
In a further 9 they were trying to evict residents.
5 were completely abandoned.
3 had been officially declared ghettos.
4 were supported in some way by the local authorities.
This is another example of different situations that develop in different ways.
We also have a further two studies from Portugal (1991) that are quite thorough providing a great deal of data from the "Greater Lisbon" area (a total of 53 neighbourhoods).
68.8% do not have running water
44.6% do not have electricity
75.9% do not have a bathroom
60.7% do not have a toilet
88.4% do not have a water heater
66.1% do not have a refrigerator
98.2% do not have heating
92.2% do not have a washing machine
32.1% do not have a gas cooker
It is important to point out that these percentages are higher than those found in the case of other marginal groups (Cape Verdians, Angolans, Guineans, etc.) that live in the same neighbourhoods. In short, the situation of the Roma population in Lisbon is sub-standard.
And finally, we have data on the different districts of Alentejo. The totals are highlighted here from a study involving 482 family homes about which a complete questionnaire was applied focusing on health, habits and living conditions (1993).
Type of dwelling
Standard 41.5%
Hovels 43.2%
Traditional-style tent 10.6%
Mobile 0.2%
Improvised 3.7%
Other 0.8%
Running water
YES 34.65%
NO 65.35%
Electricity
YES 35.7%
NO 64.3%
Sanitary installations
YES 23.2%
NO 76.8%
Bathroom / Shower
YES 21.8%
NO 78.2%
Sanitation system
YES 26.6%
NO 73.4%
In short, we once again find a very sub-standard situation. It is our belief that the data cannot be generalised to all situations but repeatedly point to the presence of segments of the population living in different places in very sub-standard conditions with regard to housing; strangely more sub-standard than those of other more recent migrant groups.
BLOCK 3: ACCESS TO THE MAINSTREAM HEALTH SYSTEM
The following five indicators were chosen at the last review of proposed indicators:
These indicators were not found in the search for secondary data. Qualitative information was found, however, on access to and use of the health system and this information is available for a number of different dates and for several geographical areas within certain countries. Some of the indicators are similar to those selected and partially cover the information provided by the latter or are somehow related thus permitting their use.
One of the indicators that appears time and again in Spain is the percentage of the Roma population that has a health card; i.e. has access to the mainstream health system. The data obtained confirm two realities:
We now turn our attention to the rest of the indicators.
The existing qualitative information shows that not all births take place in hospitals and also indicates that the length of the hospital stay is shorter in the case of Roma mothers when compared with the rest of the population.
In Madrid 10% of the births are outside of a hospital environment; the figure for Andalusia in 1985 was 62% in-hospital births. And finally, in the more developed Autonomous Communities the qualitative information shows that all births take place in health centres.
2. Relative percentage of total number of hospital emergency room visitsThere is no information on this indicator and only in an indirect fashion can it be deduced that Roma individuals tend to use emergency room services more frequently than the rest of the population given that they resort to the health system for curative purposes rather than prevention.
3. Percentage who pay visits to the family doctorThe qualitative information gathered shows that visits are infrequent (Castilla-Leon); in Galicia 38% see the doctor at least once a year while in Navarra 92% pay regular visits to health centres. These figures indicate that the Roma population use health services more frequently than non-Roma.
In the rest of the areas it was repeatedly indicated that the use of the health system is curative and not used for prevention purposes.
4. Percentage of visits to the paediatricianHere the information is similar to that obtained for indicator number 3. In Zaragoza it was stated that they do not take the children to the physician and in Granada health-care controls for children are not kept.
5. Percentage of visits to local health-care centresThe information is similar to that obtained for indicators 3 and 4 with regard to the insistence on the fact that the system is used to cure illness but no specific information was available on local health-care centre visits just as no specific information was provided for visits to the family doctor.
A summary of this block of indicators should highlight the following points:
We have chosen to group these last three indicators together (plus the one we had originally placed in Block 3 on general, dental and gynaecological check-ups) leaving just one with the general heading Doctor visits independent of the purpose of said visit. This would provide us with a visit rate that would only be distinguished from emergency-room visits.
BLOCK 4: GLOBAL HEALTH INDICATORS
As with the Block above, information gathered was scarce especially with regard to indicator number 3. We will now take a look at each indicator.
1. Percentage of stillbirthsThere is no quantitative or qualitative data regarding this indicator. In a study done in Estella (Navarra) we find the figure of 22% child mortality but this is after birth, during childhood. It also indicated that the child mortality rate was higher than that for the rest of the non-Roma population in Andalusia but no specific figures are provided.
2. Percentage of Roma over 65 years of ageAll studies show that % is very low while this figure is very high for young people; some studies also offer data on life expectancy. For Spain as a whole, Caritas provides the life expectancy figure of 52 and 62 for men and women respectively which means 20 years less than that of the rest of the population.
In Estella we find the figure of 2% of the population over 65 years of age. In Castellon life expectancy is registered as 40 and in Alentejo 6% of the population is over 60.
3. Mortality ratesMortality rate data are not provided for Spain. In Alentejo the rates are high for heart disease and infectious or contagious diseases. In general the data point to high mortality rates (15.5% in Alentejo) and some diseases are highlighted as the most prevalent causes of death.
This indicator was originally formulated in accordance with the different causes of death but in the new proposal we used the heading Mortality Rate without specifying the cause of death.
4, Percentage of deaths in childbirthThere are no references made with regard to this indicator. In this case we chose to eliminate the indicator in light of the difficulty in obtaining data and because still not all Roma women give birth in hospitals. We therefore will use this other indicator that is more primary.
In summary, with respect to this Block the lack of information is greater because the indicators are more specific. There is quite a bit of information on the percentage of elderly, on life expectancy and on overall mortality rates.
The information compiled may lead to a number of conclusions:
- Fewer visits to physicians and health centres.
- Women still give birth outside of hospitals.
- Mortality rates are higher than those observed for the non-Roma population.
- Life expectancy is therefore lower.
- The health system is used curatively and not preventively.
CONCLUSIONS
DEFINITIVE FORMULATION OF THE INDICATORS:
Block 1 Drugs
Block 2 Health habits, hygiene and nourishment
Housing utilities: Percentages of standard and sub-standard housing; running water, electricity, heat, hygienic services, etc.
Block 3 Access to mainstream systems
Percentage of births in health centres.
Proportion of Roma visits vis-à-vis the total number of hospital emergency room visits.
Percentage of Roma who visit their physician.
Block 4 Global health indicators
Percentage of stillbirths.
Percentage of the Roma population over the age of 65.
Mortality rate.
2.5. CONTINUATION OF THE PROJECT: ACTIONS ENVISIONED
In proceeding ahead with the development of the Information System, we foresee the following actions:
Through these actions we will continue developing the system and, by means of the Delphi studies, a global vision will be obtained on the situation and health status of the Roma in each one of the countries. We also feel that it is very important to begin to set up information collection systems whether these be through the collection of health data on Roma in already-existing systems (drug centres, health centres, neighbourhood clinics) or through the programs that are being carried out by the participating organisations or other organisations that decide to take part.